Visual answer
Can an Eye Be Donated: the idea in one diagram
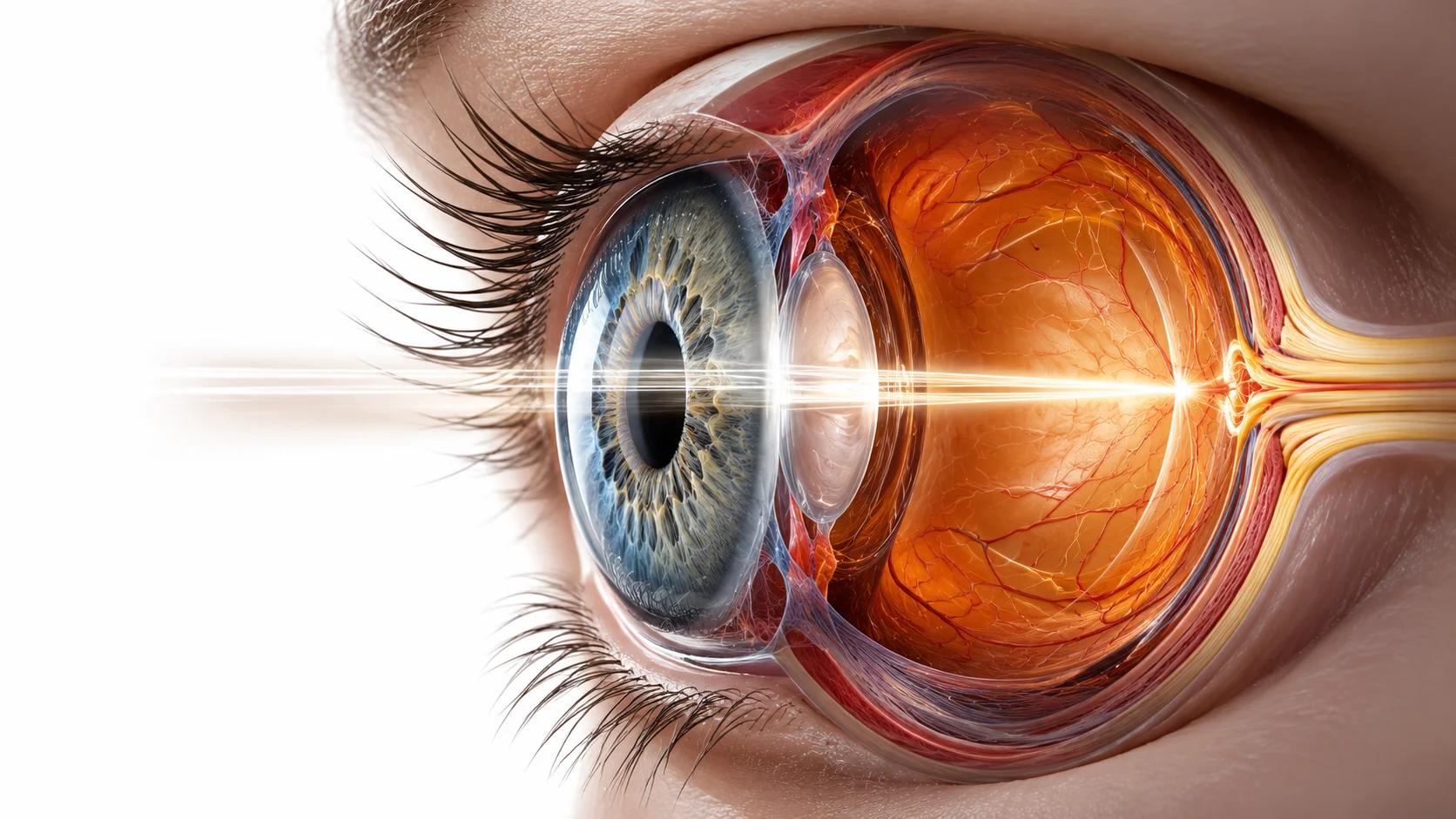
Eye donation works because transplant medicine uses specific eye tissues, especially the cornea, rather than replacing the whole eye. The optic nerve still cannot be reconnected, but corneal layers can be recovered, preserved, matched to the recipient's disease, and transplanted with high success.
Donor tissue is recovered
Donation begins with careful tissue screening, not whole-eye replacement.
The needed layer is prepared
Most modern corneal donation is targeted layer repair.
The recipient's damaged tissue is replaced
Sight is restored by repairing the eye's clear optical surface.
Answer
The Direct Answer
Specific parts of the eye, particularly the cornea and sclera, can be donated and transplanted successfully. The whole eye as a complete organ cannot currently be transplanted because the optic nerve cannot be reconnected.
Eye banks retrieve eyes from donors within hours of death, evaluate the tissue quality, and process specific layers for transplantation. The cornea, the clear front surface of the eye, is the most commonly transplanted part and restores sight in thousands of patients annually. Modern surgical techniques can transplant individual layers of the cornea rather than the full thickness, dramatically improving outcomes. The retina and optic nerve, which connect to the brain, remain outside current transplant capability.
The cornea, a transparent disc of tissue roughly the size of a shirt button, has no blood vessels and is immunologically privileged, meaning the body is far less likely to reject it than almost any other transplanted tissue. This quirk of anatomy has made corneal donation one of the most successful and routine forms of tissue transplantation in medicine.
Big questions
The Questions That Make It Interesting
These are the pressure points of the idea: the places where the simple answer becomes a much stranger story.
Why can't the whole eye be transplanted?
The optic nerve, which connects the retina to the brain, cannot currently be reconnected after severance. The retina processes visual information and transmits it as electrical signals through the optic nerve to the visual cortex. Cutting and reattaching the optic nerve destroys the connection irreversibly. Without optic nerve reconnection, a transplanted eye would be anatomically present but functionally blind.
The same neural reconnection problem that prevents brain transplantation also prevents whole-eye transplantation, just with a smaller but still unresolvable number of nerve fibers.
What is a DMEK transplant and why has it changed corneal surgery?
DMEK (Descemet Membrane Endothelial Keratoplasty) is a technique that transplants only the innermost cellular layer of the cornea, approximately 10 to 15 microns thick, from a donor. It replaces only the diseased endothelial cells rather than the full corneal thickness. The technique produces dramatically faster visual recovery, much lower rejection rates, and better final visual acuity than previous full-thickness transplants.
Modern corneal transplantation has become so precise that surgeons are transplanting tissue layers thinner than a human hair with reliable success.
Can corneal tissue be grown in the lab?
Research into bioengineered corneas is active and producing promising results. Lab-grown corneal endothelial cells have been transplanted successfully in small clinical trials. Collagen-based scaffolds seeded with corneal cells have been tested in humans in some countries. A fully functional synthetic cornea that matches donor tissue in all properties does not yet exist but is an active research goal given the worldwide shortage of donor corneas.
There are 12 million people worldwide waiting for a corneal transplant with no available donor. A bioengineered solution would be one of the most impactful interventions in global ophthalmology.
Surprises
The Surprising Details
Surprising fact
A single eye donor can restore or improve the sight of up to five people through different uses of the donated tissue.
Surprising fact
The cornea has no blood supply, receiving oxygen directly from the air and nutrients from the aqueous humor. This makes it immunologically privileged and dramatically reduces rejection risk.
Surprising fact
Corneal tissue remains viable for transplantation for up to two weeks after donation if stored in specialized preservation media, far longer than hearts or kidneys which must be transplanted within hours.
Counterintuitive finding
Older donor corneas are often preferred over younger ones for certain types of transplants because the cellular density of the endothelial layer at the back is sufficient, and surgeons know exactly what they are getting.
Counterintuitive finding
Most corneal transplants today use only a fraction of the cornea, transplanting a single targeted layer rather than the full thickness, dramatically improving recovery time and reducing complications.
Counterintuitive finding
The most common cause for corneal transplantation is not injury or infection but Fuchs' dystrophy, a hereditary degeneration of the corneal endothelium that causes it to gradually pump less fluid and cloud the vision from the inside out.
Fascinating comparison
Corneal transplantation is now as precisely targeted as replacing a single pane in a multi-layer window, rather than replacing the entire window frame.
Fascinating comparison
The immunological privilege of the cornea makes it almost unique among transplanted tissues. Transplanting it is closer to transplanting a contact lens made of biological material than to transplanting a kidney.
Everyday example
Many people with Fuchs' dystrophy, who notice their vision becoming progressively hazier over years, are unaware that they are candidates for a routine corneal transplant with high success rates and relatively rapid recovery.
Everyday example
Corneas from the same donor can be split and prepared for different types of recipients depending on the condition being treated.
Mechanism
How It Actually Works
Eye donation works because transplant medicine uses specific eye tissues, especially the cornea, rather than replacing the whole eye. The optic nerve still cannot be reconnected, but corneal layers can be recovered, preserved, matched to the recipient's disease, and transplanted with high success.
- 1
Donor tissue is recovered
After death, an eye bank retrieves and evaluates the donated eye tissue under sterile conditions, checking corneal clarity, cell density, safety, and suitability for transplant. Analogy: It is like inspecting an optical lens before deciding whether it can be used in a precision repair. Takeaway: Donation begins with careful tissue screening, not whole-eye replacement.
- 2
The needed layer is prepared
Depending on the recipient's condition, technicians may prepare a full-thickness corneal graft or only a thin endothelial layer such as DMEK tissue. Analogy: Modern corneal surgery can replace one damaged pane in a layered window instead of replacing the whole window. Takeaway: Most modern corneal donation is targeted layer repair.
- 3
The recipient's damaged tissue is replaced
The surgeon removes the diseased corneal tissue and positions the donor tissue so light can again pass cleanly through the front of the eye. Analogy: The repair is closer to changing a camera lens element than transplanting an entire camera. Takeaway: Sight is restored by repairing the eye's clear optical surface.
Story
The Story Behind the Science
The First Corneal Transplant, 1905
Eduard Zirm, an Austrian ophthalmologist, performed the first successful human corneal transplant in 1905, taking a cornea from an 11-year-old boy whose eye had been removed due to injury and transplanting it into a farm laborer who had been blinded by chemical burns.
The patient recovered useful vision and retained it for years. Zirm's operation, which preceded the discovery of blood groups and the development of anti-rejection drugs by decades, succeeded because the cornea's lack of blood vessels meant the immune system never launched the full rejection response that would have destroyed any other transplanted tissue. The first successful organ or tissue transplant in human history succeeded partly because the surgeon, perhaps without fully understanding why, chose the one tissue in the body that the immune system was least likely to attack.
Establishment of the first eye bank, 1944
The Eye Bank for Sight Restoration was established in New York City in 1944, creating the infrastructure to collect, store, and distribute donor eye tissue systematically for the first time.
Before organized eye banking, corneal transplants were ad-hoc procedures requiring a conveniently timed donor. The eye bank model transformed them into scheduled, reproducible surgery and established the template for all subsequent tissue banking.
Evidence
Experiments and Evidence
Development of DMEK by Melles et al., 2006
Dutch ophthalmologist Gerrit Melles developed the technique of transplanting only the Descemet membrane and endothelial layer of the cornea, a mere 10 to 15 microns of tissue, rather than full-thickness corneal buttons.
Patients achieved better final visual acuity, recovered faster, and had significantly lower rejection rates than with previous techniques. DMEK is now the preferred approach for endothelial diseases like Fuchs' dystrophy in most major centers worldwide.
Pattern
The Deeper Pattern
The cornea is less than half a millimeter thick and has no blood vessels at all, fed entirely by diffusion of oxygen from the air and from surrounding fluids. It is simultaneously one of the most sensitive tissues in the body, with among the highest nerve density of any structure, and one of the most tolerant of transplantation.
The body part with the most nerve endings per square millimeter is also the one most likely to be successfully transplanted without rejection.
Global demand for corneal transplants exceeds supply by approximately 70 to 1. For every donor cornea available, 70 patients are waiting.
Corneal donation is one of the simplest and most impactful things a person can do, and the shortage is driven primarily by low awareness rather than medical limitations.
The success of corneal donation rests on a structural biological anomaly: the cornea evolved to be avascular to maintain optical clarity, and that same absence of blood vessels eliminated the immune surveillance that causes rejection in other transplanted tissues.
Evolution made the cornea transparent by removing its blood supply, and in doing so, accidentally made it the most transplant-friendly tissue in the body. Biology's optical solution became surgery's ethical windfall.
The properties most useful for one purpose sometimes create unexpected advantages in entirely different contexts.
Edge cases
Where the Rule Gets Weird
Keratoconus: corneal thinning in young adults.
Keratoconus is a condition where the central cornea thins and bulges forward into a cone shape, severely distorting vision. It affects roughly 1 in 2,000 people, often developing in the teenage years. In severe cases, corneal transplantation is the only treatment. These younger patients often receive full-thickness or anterior lamellar transplants because they need structural replacement, not just endothelial cell restoration.
Keratoconus makes corneal transplantation necessary in otherwise healthy young people, and the long-term success of their transplants is a testament to the cornea's immunological privilege.
Myths
Myths vs Reality
Eye donation leaves the donor's body without eyes, which is disfiguring.
Eye banks remove the cornea or the entire eye under sterile conditions and can restore the donor's appearance with prosthetic shells before the funeral. The process is not visible at a viewing.
Standard eye donation protocols specifically address cosmetic concerns to maintain the option of open-casket funerals.
Doctors might not try as hard to save you if you are a registered eye donor.
This is the most common misconception that discourages registration. Eye banks are completely separate from emergency and critical care medicine. The decision to declare death and the decision to request donation are handled by different teams under strict protocols.
Legal and hospital protocols in all countries with organized donation systems require that the care team and the donation team operate independently.
Real world
What This Changes in Real Life
Registering as an eye donor takes approximately two minutes and could restore the sight of up to five people. The gap between available donor corneas and patient need is driven almost entirely by low registration rates, not by medical or logistical barriers.
Countries with opt-out donation systems, where citizens are presumed to consent unless they actively withdraw, have significantly higher donation rates and shorter waiting lists than opt-in systems.
Takeaways
Key Takeaways
Takeaway 1
Parts of the eye, especially the cornea, can be donated and routinely restore sight.
Takeaway 2
The whole eye cannot be transplanted because the optic nerve cannot be reconnected.
Takeaway 3
The cornea's lack of blood vessels makes it uniquely resistant to immune rejection.
Takeaway 4
A single donor can help restore or improve the sight of up to five people.
Takeaway 5
Global demand for corneal transplants exceeds supply 70 to 1, primarily due to low donor registration.
Quick answers
Common questions
Why can't the whole eye be transplanted? +
The optic nerve, which connects the retina to the brain, cannot currently be reconnected after severance. The retina processes visual information and transmits it as electrical signals through the optic nerve to the visual cortex. Cutting and reattaching the optic nerve destroys the connection irreversibly. Without optic nerve reconnection, a transplanted eye would be anatomically present but functionally blind.
What is a DMEK transplant and why has it changed corneal surgery? +
DMEK (Descemet Membrane Endothelial Keratoplasty) is a technique that transplants only the innermost cellular layer of the cornea, approximately 10 to 15 microns thick, from a donor. It replaces only the diseased endothelial cells rather than the full corneal thickness. The technique produces dramatically faster visual recovery, much lower rejection rates, and better final visual acuity than previous full-thickness transplants.
Can corneal tissue be grown in the lab? +
Research into bioengineered corneas is active and producing promising results. Lab-grown corneal endothelial cells have been transplanted successfully in small clinical trials. Collagen-based scaffolds seeded with corneal cells have been tested in humans in some countries. A fully functional synthetic cornea that matches donor tissue in all properties does not yet exist but is an active research goal given the worldwide shortage of donor corneas.